

What is a pneumothorax?
When air leaks out of the lung it collapses and leaves a space around it. The medical term for a collapsed lung is a pneumothorax. A small pneumothorax will often heal by itself, however sometimes they don’t heal up or they come back. A chest drain may be used at first but if this fails an operation may be needed to help re-inflate the lung and stop it collapsing again. If you have had a pneumothorax more than once, surgery is intended to help prevent this happening again.
Thoracic surgeons look after patients who need surgery for a pneumothorax. They also look after patients who have a pneumothorax that is difficult to treat, even if they do not need surgery.
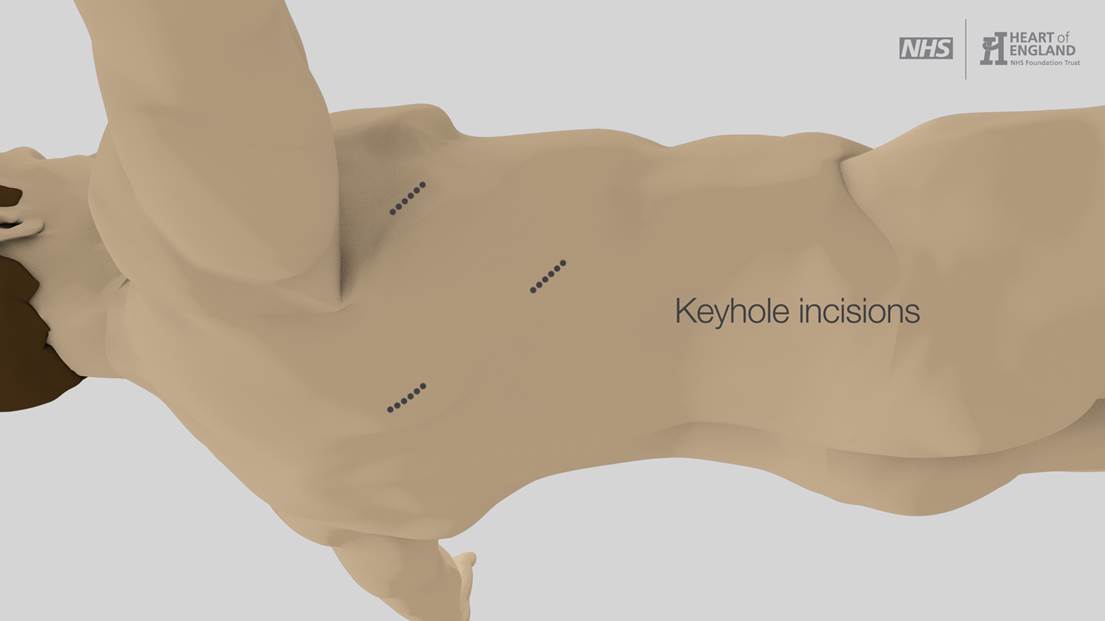 A number of techniques can be used to fix a pneumothorax. There are two parts to the surgery; dealing with area of lung that has leaked and preventing the pneumothorax from coming back. These procedures are done as keyhole (VATS) surgery. VATS stands for Video Assisted Thoracoscopic Surgery.
A number of techniques can be used to fix a pneumothorax. There are two parts to the surgery; dealing with area of lung that has leaked and preventing the pneumothorax from coming back. These procedures are done as keyhole (VATS) surgery. VATS stands for Video Assisted Thoracoscopic Surgery.
During surgery you lie on your side with your arm raised. Up to 4 small cuts are made, each about 5cm (2 in) long. These are used for the instruments and small camera to go into the chest. Special staples are used to cut and seal any parts of lung that need to be removed. The piece of lung can be removed through one of the small cuts. The wound is closed with dissolvable stitches. 1 or 2 chest drains are put in at the end of the operation and held in placed with a stitch. These remove any fluid or air from around the lung.
If a part of the operation cannot be done keyhole the operation may need to be changed to the open technique (thoracotomy). Open surgery is done with one longer cut under the shoulder blade between 2 ribs. The 2 ribs are parted to get into the chest. One rib may be cut to give more space, ribs are not removed. At the end of surgery the 2 ribs are held back together with strong stitches. The muscles and skin are also stitched back together.
If you have had repeated episodes of pneumothorax or you wish to do scuba diving your surgeon may decide it is best to use the open technique to do your operation.
- Dealing with area of lung that has leaked
Bubbles of thin lung tissue around the edge of the lung can be the cause of a pneumothorax if they burst. A small bubble is called a bleb, a large bubble is called a bulla. Removing these abnormal parts of the lung helps stop air leaking out of the lung. Removing such a small amount of lung does not give you any long term breathing problems.
- Preventing the pneumothorax from recurring
If the lung becomes stuck to the inside of the chest wall there is less chance of the lung collapsing. Removing the pleura on the inside of the ribs makes the inside of the chest wall sticky. This causes the lung to stick to chest wall. Alternatively sterile talc powder can be put into the chest usually during the operation. The powder causes irritation which makes the lung stick to the chest wall. The lung sticking to the chest wall is called pleurodesis.